heart-lung machine
[′härt ′ləng mə‚shēn]Heart-Lung Machine
an apparatus that ensures an optimal level of blood circulation and metabolic processes in the body of a patient or in an isolated donor organ, intended for the temporary performance of the functions of the heart and lungs.
On the basis of numerous previous works, the first apparatus for artificial blood circulation of a warm-blooded animal—the autojector—was created in 1925 by the Soviet scientist S. S. Briukhonenko. The Soviet scientist N. N. Terebinskii proved the possibility of successful heart-valve surgery with the aid of this apparatus in 1930. In 1951 the Italian surgeons A. Dogliotti and A. Costantini surgically removed a tumor of the mediastinum while using a heart-lung machine. The first operation in the USSR on a “dry” heart with the aid of a heart-lung machine was performed in 1957 by A. A. Vishnevskii.
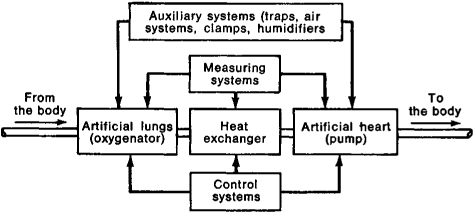
The heart-lung machine is a complex of interconnected systems and units: an artificial heart—an apparatus consisting of a pump, drive mechanism, and transmission that delivers blood at a bulk speed of flow sufficient to ensure life; and artificial lungs—a gas-exchange device (an oxygenator) that serves to saturate the blood with oxygen, remove carbon dioxide, and maintain the acid-alkaline balance within physiological limits. The oxygenators may be constructed according to one of four principles of oxygen saturation: bubble, film, froth-film, and semipermeable synthetic membrane. A model of a froth-film oxygenator was created by Briukhonenko and V. D. Iankovskii in 1937; it is the froth-film principle that is principally used in Soviet oxygenators, which in their functional qualities are more “physiological” than oxygenators that operate through the direct contact of respiratory gases with the blood.
Three types of blood pumps are used: those that produce the systole and diastole separately, based on changes in the chamber volume produced by a diaphragm with the aid of a hydraulic or pneumatic agent; those that create blood flow in flexible tubes through dilation or contraction, the valves being located either outside the tubes or within the bores, and those that produce blood flow in intermittent waves (roller and finger pumps). All blood pumps are divided into constant and variable stroke-volume types, according to mechanism of action, and into small-and large-pulsation types, according to the nature of the blood flow they produce. In order to maintain temperature regimes appropriate to the purpose of the operation, that is, in order to conduct artificial blood circulation at normal or lowered temperatures, a heat exchanger with a thermoregulating device is used. A control system ensures the set operating conditions for both the separate functional units and the total apparatus. The heart-lung machine is driven by hydraulic, pneumatic, or electromechanical mechanisms. A manual drive is used in emergencies.
More than a hundred types of heart-lung machines have been developed throughout the world for various purposes, such as for the isolated chemotherapy of malignant neoplasms, inflammatory processes, and destructive lesions; for auxiliary artificial blood circulation in serious disturbances of cardiac and respiratory functions; for resuscitation in cases of clinical death; and to maintain the vital activities of isolated organs that are intended for subsequent transplant. All of these machines have a common structural plan, but they differ from one another in capacity, in features of their control systems, or in the inclusion of special supplementary functional units. Systems for hooking up the heart-lung machine to the patient’s vascular system depend on the type of artificial blood circulation selected. Heart-lung machines used in heart surgery commonly use an artificial heart of roller pumps and artificial lungs of a disk oxygenator (the American Pemco, Sarens, and Imico models and the Soviet ISL-4 and ASP-2). In the Soviet models (the AIK-5 and the AIK-5M), the physiological unit consists of diaphragm pumps and a froth-film oxygenator.
REFERENCE
Galletti, P. M., and G. A. Brecher. Osnovy i tekhnika ekstrakorporaV-nogo krovoobrashcheniia. Moscow, 1966. (Translated from English.)N. A. SUPER